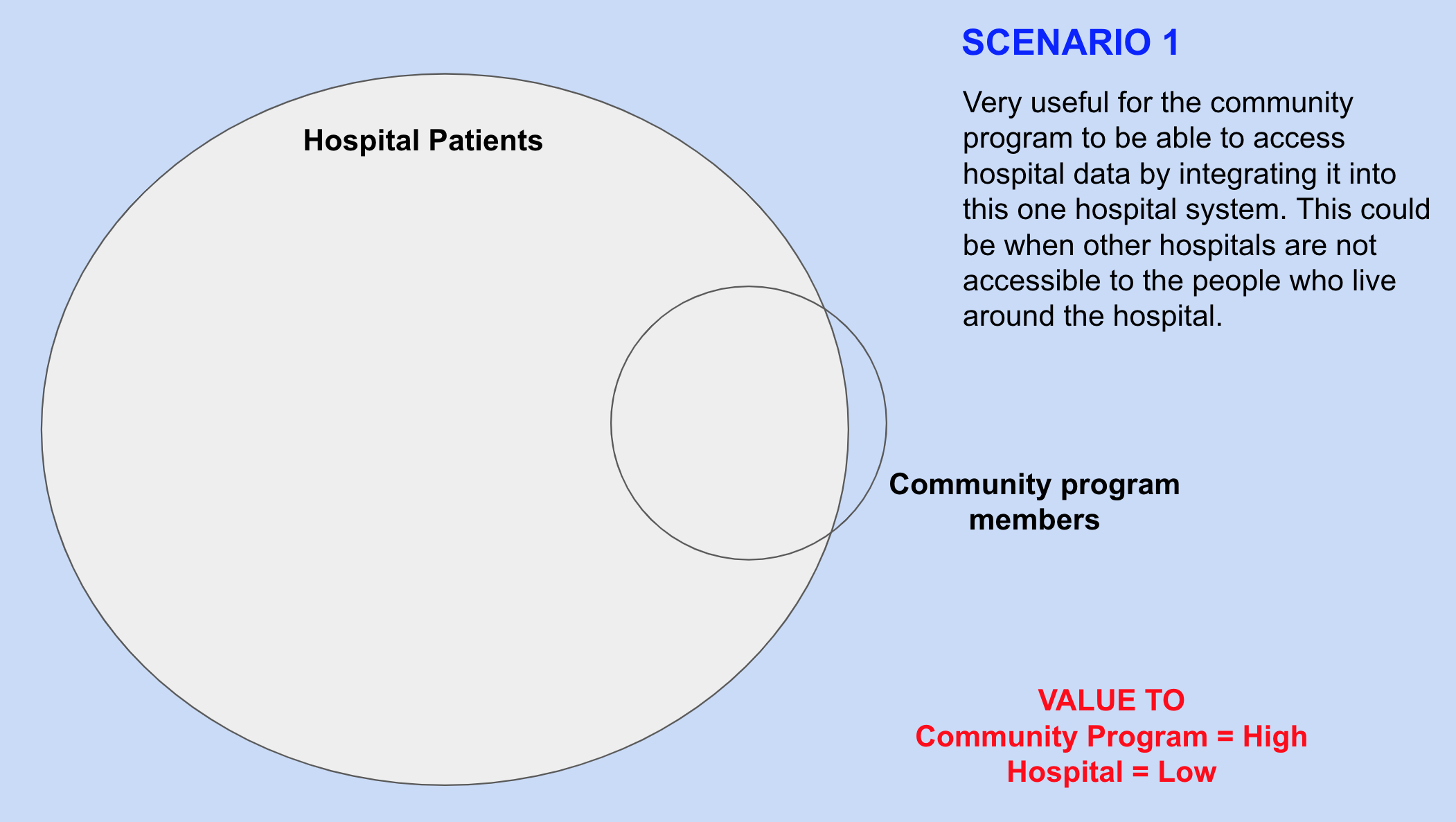
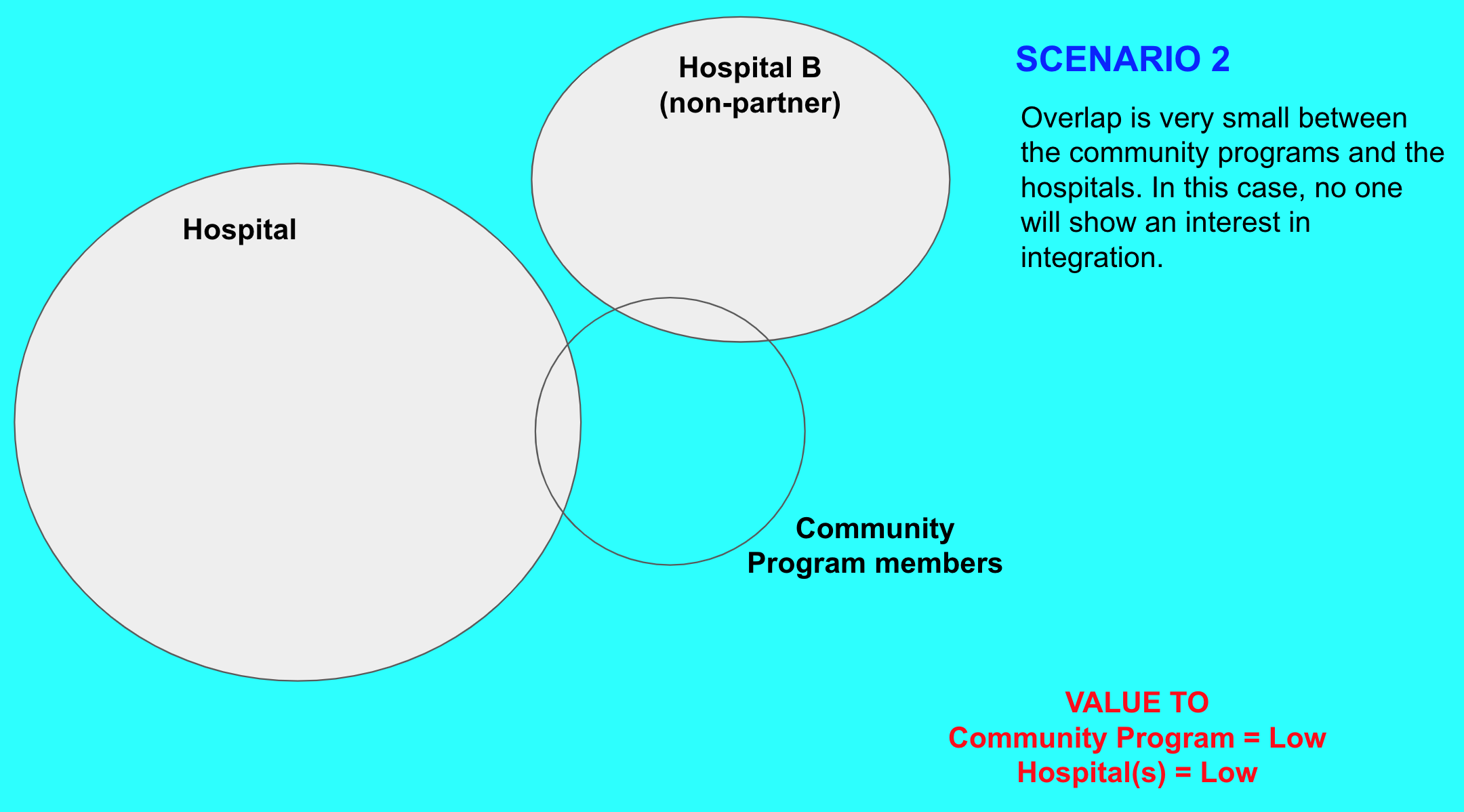
The main objective of the integration of data between hospital and community programs is to make the patient/member health data accessible to the counterparties - so that better health services can be provided to them. This is explained in more detail here. For the integration between these software systems to be of value let's consider the following four scenarios.
Common Identifier
It is perhaps obvious, but if this data has to be made available across these systems then we need an individual identifier (ID) or a reliable set of fields that can be used to link records. In Ashwini's case, community members are provided an ID in the community by the health workers. If the patient brings their ID card with them to the hospital then the hospital uses the same ID to register the person by putting some prefix to it which separates such patients from non-community patients.
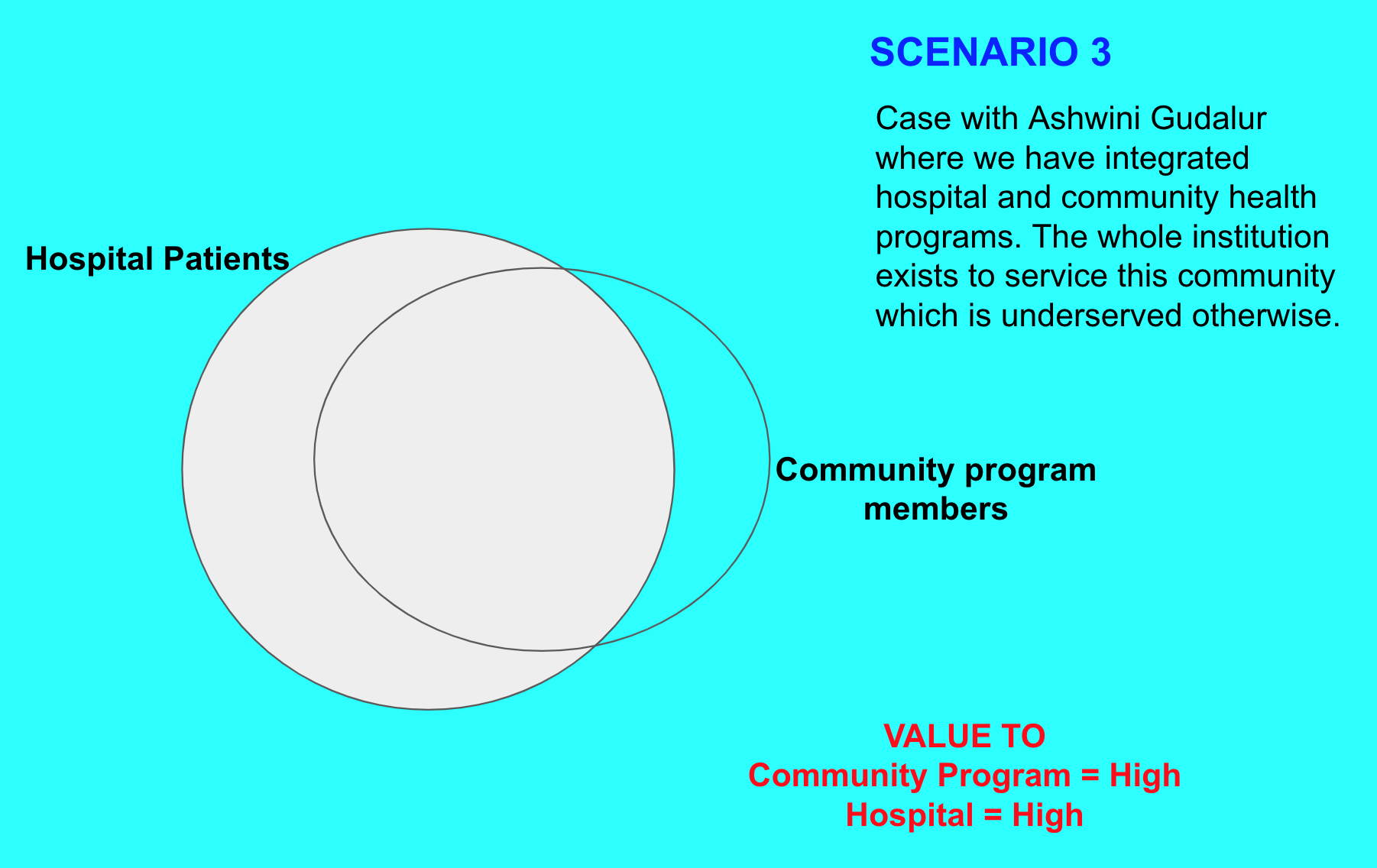
Let's assume for the rest of this writeup that we have scenario 3 above as that allows us to explore all other issues that we may have to deal with - which may not arise in other scenarios.
Should a community member be automatically registered as a hospital patient by the integration process - if they are not present?
Automatically registering a patient in a hospital system may confuse the registration and hospital administration department - when the patient in future visits the hospital for the first time. It will also inflate the number of patients registered with the hospital, used for operational planning. Bahmni allows for keeping individual records without registration with the hospital - this provision is quite useful because if and when such patient visits for the first time, his/her community records will be ready to use after registration.
Now let's look at the reverse.
If there is a patient in the hospital but not present in the community program - should such a patient be automatically registered. Intuitively, we should follow the same as above but if a community program is where ID is provided then a member not existing indicates that something is wrong and hence better resolved manually.
Do not synchronize - Lab, Radiology Orders, and other workflow-related data
We decided that making these available in the community health system is not of much value. What community health workers will require is the results, not the order information. The order information is really about the workflow within the hospital. An even simpler example is if the hospital provides a token number to the patient, it is not all that relevant to anyone after the patient leaves the hospital. Making such records available in the community health system is not very useful.
For the inpatient, records synchronize only discharge summary
Making the outpatient clinical records available to the community health worker is quite useful. But when a patient is admitted to a hospital the s/he is prescribed and administered several medicines and many tests are conducted. We thought that making all these drug orders and lab results available to the community health worker is not going to be helpful (too much detail, perhaps also requires deeper clinical understanding to make sense of it). As in the same way, a patient rarely uses/requires such inpatient records after one is discharged. Patients mainly use discharge summaries. We decided to do the same for the integration, i.e. in case of inpatient visits, we synchronize discharge summary with the community health system and leave out drugs administered and lab results.
Hospital record drives the workflow of CHW, but the reverse is not true
Let's say if a woman delivers in the hospital. When she is discharged the CHW should follow up with her (and her child) for post-natal care (PNC). This implies that there must a be mechanism by which CHW can find out this information. There are a couple of features in Avni (the CHW system) that help here - Avni provides a dashboard where CHW can find such women from their catchment and perform the next step. Avni android app performs periodic auto-sync which ensures that hospital records are made available at the earliest.
The follow-up within the community after someone comes back from the hospital to CHW needs to be supported digitally because CHW's role is to provide proactive care. The same is not true for the hospital. Hospitals typically provide care only when a patient visits the hospital. Hospitals are not structured to provide proactive health services. In fact, the workflow from the CHW to the hospital is also facilitated by the CHW - by asking patients to visit the hospital. Hospitals are reactive setups.
To summarise the integration between community health and the hospital system should be based on understanding how patients behave and how community programs and hospitals operate. Lastly, the integration should leave difficult decisions of deduplicating individuals, deleting records, when to register, when to enroll in or exit from disease programs to the humans - because doing them automatically can create difficult-to-resolve data problems and may impact health services provided to an individual. Following do no harm is a good thumb rule.
Author: Vivek Singh
Date: 03-Sept-2021